Liposarcoma
It is one of the most common malignant tumors of the adult. It correspondsto 2.5 patients per million and 9.8 to 16% of soft tissue sarcomas. In the same group of liposarcomas there are a wide variety of subtypes, different from each other and with behavior from non-metastatic ones (e.g.: atypical lipomatous neoplasia) to highly metastatic ones (e.g.: pleomorphic liposarcoma). All liposarcoma subtypes have certain characteristics in common, such as deep localization in contrast to lipomas that are superficial and rarely occur in children.
Lipossarcomas are currently subdivided into:
- Well differentiated liposarcoma
- Liposarcoma lipoma-like
- Inflammatory liposarcoma
- Sclerosing liposarcoma
- Myxoid Liposarcoma
- Pleomorphic liposarcoma
- Pleomorphic myxoid liposarcoma
- Dedifferentiated Liposarcoma
- Epitelioid Liposarcoma
They are tumors derived from malignant lipoblasts. They affect any tissue in which fat is present and, in general, are malignant since its appearance. They present great variation of behavior, of low degree, well differentiated, up to high grade, with round and pleomorphic cells. They rarely originate from pre-existing lipomas. Several pathologists do not accept the thesis of malignancy of lipomas in liposarcomas.
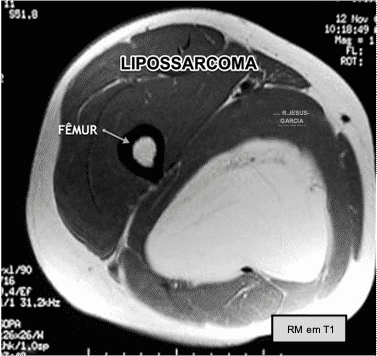
They appear at all ages, but the peak incidence is from 40 to 60 years. The most common locations of appearance are the lower limb, the abdominal cavity, the retroperitoneum, the trunk, the upper limb, the head and neck in descending order.
Sometimes, they can be multicenter, especially in the abdominal cavity. They are painless and can reach large volumes without the patient noticing their presence and growth.
Pathology
Macroscopic examination of the resection piece reveals that they are usually large, with a lobulated surface, with an aspect reminiscent of the cerebral cortex. Sometimes, they can take on aspects of dumbbells when they are presented with tablets by fibrous structures. Other times, there may be, especially in retroperiton tumors, more than one discontinuous lobe with the main mass. At the cuts the tumor is yellow-whitish, with firmer consistency when it contains a large amount of fibrous tissue, but more often softened when adipose and myxoid tissue predominates. Areas of necrosis are common in large-volume tumors.
Histologically, close to 50% are myxoid liposarcomas, characterized by lipoblasts, with branched and extremely thin capillaries, in the middle of the myxoid matrix. Poorly differentiated myxoid liposarcoma composed of small cells exhibits a more aggressive behavior, despite the rarity of atypical mitoses. This pattern is common in liposarcomas that present recurrence. Well differentiated liposarcomas have a pattern similar to lipomas, but with great variation in the size and shape of the nuclei. In addition, they may contain undifferentiated areas. Pleomorphic liposarcomas are characterized by the presence of large giant cells, which may contain fat drops.
Liposarcoma Treatment
Treatment of liposarcomas consists of resection of the tumor with wide margins. Adjuvant treatment in high-grade malignancy tumors should always be discussed with clinical oncologists to assess the advantages and disadvantages of chemotherapy, especially in older patients. In recent years, studies have been conducted to evaluate the efficacy of immunotherapy in the treatment of liposarcomas. However, the use of anti PD-L1 drugs (pembrolizumabe) only showed effectiveness in the subtype of dedifferentiated liposarcoma.
Liposarcomas are among the most radiosensitive tumors among sarcomas. Based on this high sensitivity, we indicate, in our Service, radiotherapy for all patients with high-grade liposarcomas.
In some cases, high-grade liposarcoma may be treated with brachytherapy as an alternative to external radiotherapy. In patients with inadequate surgeries with contaminated margins or in cases of recurrence, brachytherapy can be used at the time of surgery to review and enlarge the margins.
Liposarcoma Prognosis
The most important prognostic factor for liposarcomas is anatomical localization. Lesions located in regions accessible to surgical resection have a low recurrence rate (< 2%) complete resection with wide margins. However, tumors that are located in regions of difficult surgical access, such as retroperitoneum or mediastinum, usually present high rates of local recurrence (> 20%), mainly due to surgeries with marginal or contaminated margins. Usually evolve with local complications or with dedifferentiation after several surgeries and the appearance of metastases.
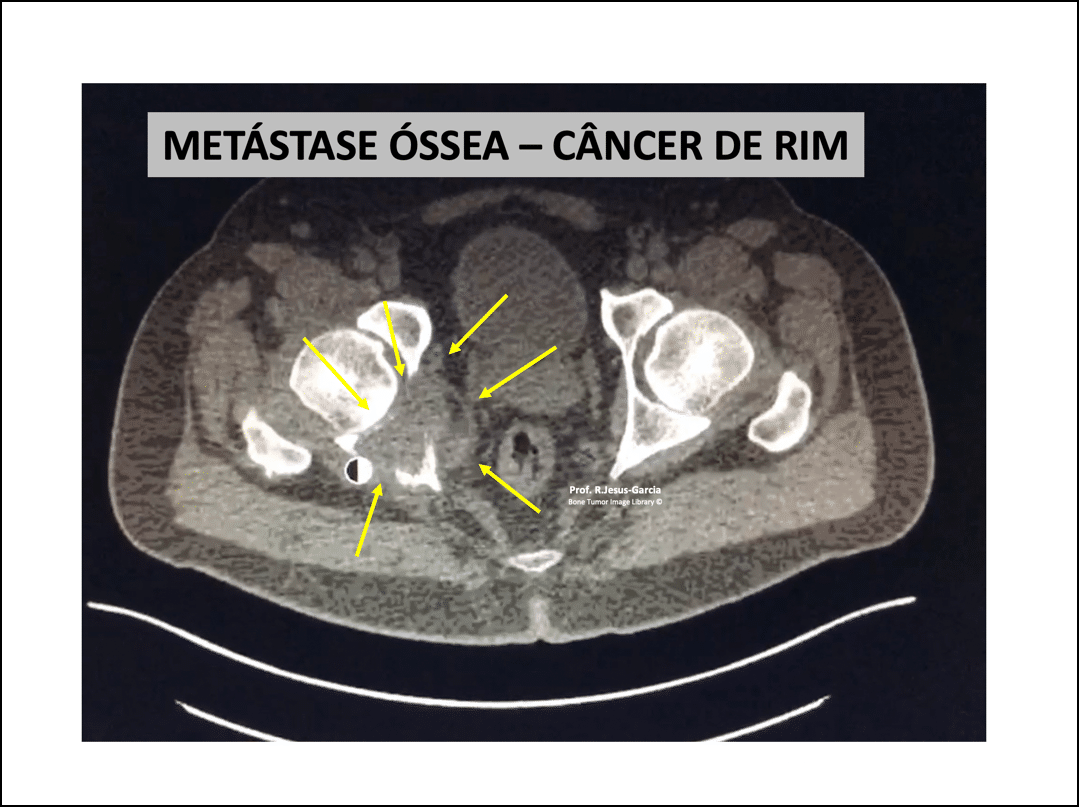
Overall liposarcoma survival ranges from 100% survival in atypical lipomatous tumors to 20% survival at 10 years in dedifferentiated liposarcomas located in retroperitoneum or mediastinum. Liposarcomas have a predilection for pulmonary and bone metastases.
Myxoid Liposarcoma
It is a malignant tumor of unknown etiology and composed of uniform round or ovoid cells, with variable number of lipoblasts, located in a myxoid stroma, with a capillary vascularization network (“chicken web”). They present mytotic activity and high degree of nuclear. They represent about 5% of soft tissue sarcomas and 20-30% of liposarcomas. Its peak incidence is in the 4th decade. It is the most common type of Liposarcoma of children and adolescents. It is located in the deep tissues of the extremities. It can rarely develop primarily in the subcutaneous or retroperitoneum.
Clinical Aspects of Myxoid Liposarcoma
They present themselves as large and painless masses. In retroperitoneum, they are usually not primary but metastasis from other locations. The multifocal presentation, either synchronous or metachronous, represents distant soft tissue metastasis of monoclonal origin.
Diagnosis by Molecular Pathology of Myxoid Liposarcoma
Demonstration of translocation/fusion transcription may be useful in differentiating myxoid liposarcoma from other myxoid sarcomas and round cell sarcomas. FUS and EWSR1 transcription may occur in other sarcomas, but the DDIT3rearrangement (FUS-DDIT3) or EWSR1-DDIT3 fusion genes are pathognomonic of Myxoid Liposarcoma. Because of this, in FISH, break-apart probes directed at DDIT3 are a specific sensitive strategy.
Treatment of Myxoid Liposarcoma
Surgical resection is the treatment of choice. However, myxoid liposarcoma is extremely radio sensitive.
As regards drug treatment, it is relatively sensitive to anthracyclics (examples: doxorubicin, epirrubicin) and trabectedin.
With regard to neoadjuvant treatment, we found a marked decrease in cellularity, both in chemotherapy and preoperative radiotherapy, with only scant ovoid cells, stromal hyalinization and sometimes maturation in white adipose tissue.
Prognosis of Myxoid Liposarcoma
Local recurrence occurs in 12-25% of patients, with metastases in approximately 30-60% of patients, sometimes years after initial diagnosis and may progress slowly. They may develop bone (spine) or lung metastases. Histologically tumors with a higher degree of malignancy (>5% hypercellularity) have a higher risk of metastases and death.